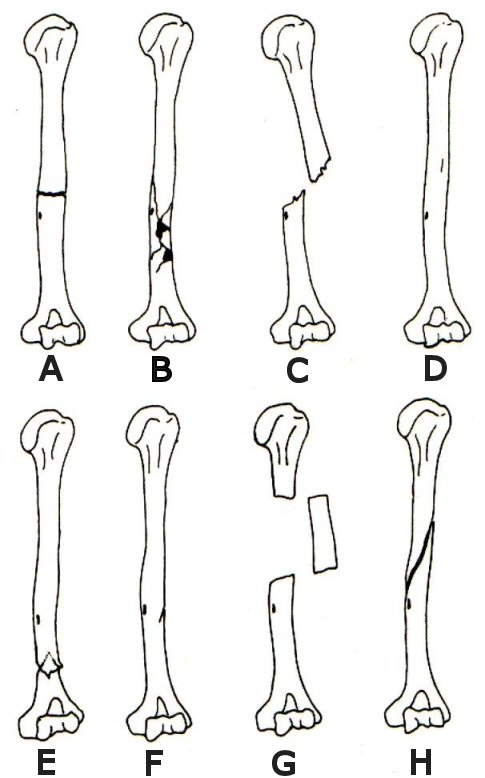
Figure 2: Types of long bone fracture (Mann and Murphy 1990 fig. 97)
Figure 1 represents a downloadable form that can be used to describe the pathological features observed on post-cranial skeletal elements, with a completed example seen in Figure 3, based on a specimen illustrated in Figures 4 and 5. What follows is a description of the principal elements included within that form. As noted earlier, one critical aspect of a recording system for pathology is to provide a precise location for the lesion using anatomical terminology. Such information is required not only to aid in differential diagnosis and to record the extent of the lesion, but is essential if the prevalence of particular pathologies is to be established. Recent years have seen the adoption of a number of zoning systems (e.g. Dobney and Reilly 1988; Serjeantson 1996). Such systems are ideally suited to the recording of palaeopathological lesions since each bone is divided into a series of anatomically unique zones. Moreover, the use of such systems by faunal analysts is already widespread (e.g. Albarella and Serjeantson 2002; Outram et al. 2005). Other factors to be recorded include taphonomic condition, to indicate whether post-depositional processes might have affected the appearance or extent of any pathological lesion; as with the diagnostic zones, these should follow published criteria (e.g. Harland et al. 2003) or be clearly stated.
The recording methodology emphasises the description rather than the diagnosis of pathologies. However, in order to describe bone lesions adequately it is necessary to have some knowledge of the biology of bone disease. While space does not allow this to be detailed fully here, it is outlined elsewhere (e.g. Reid and Roberts 2005). The protocol was thus based upon the four main types of bone reaction. These fall into two broad categories, the first being some type of disturbance in the growth and development process resulting in abnormal size and shape, and the second being secondary abnormalities imposed upon previously normal bone which stimulate bone formation or destruction. However, these descriptive categories are not mutually exclusive or discrete (Ortner 1994, 74). For this reason it was considered necessary to keep them separate, permitting the user to describe more than one, if appropriate, for each lesion.
Alteration in size should be simply recorded as whether the abnormality was an enlargement or reduction of the norm. With regards to the alteration in shape it should be noted whether this was due to bowing, expansion of the shaft, articular extension, displacement, thickening of the epiphyseal plates or some other means.
Once the type of bone formation has been defined, aspects such as the size, extent, general shape of the lesion and, where possible, the nature of the margin between the normal and abnormal bone can be described. This is important because pathologies that present well-defined margins of dense compact bone are the result of a relatively slow process. Conversely, those with porous, less well-organised, bone are faster forming and often more aggressive, or have not had time for repair to take place (Ortner 1994, 75). In addition to this information, a description of the interior of the lesion and the presence or absence of sclerosis (if an X-ray has been taken of the bone to permit this) should be recorded where possible. This not only provides a detailed description, but also gives some indication of the nature of the condition concerned, which can be used later during the differential diagnosis.
Fractures were placed in a separate category, both because they are common and also for the sake of simplicity given the number of variables specific to them. These variables relate to the nature of the force and the osseous area of distribution of the force. Factors such as magnitude, direction, loading, rate and duration determine the impact of the force, while susceptibility is determined by bone density, fatigue strength, resilience and elasticity (Rothschild and Martin 1993, 51). The form therefore records the type of fracture seen, as well as the angle and direction of any resulting deformation or foreshortening. The presence or absence of any evidence of healing should also be noted.
Figure 2: Types of long bone fracture (Mann and Murphy
1990 fig. 97)
As illustrated in Figure 2, there are several types of fracture (Mann and Murphy 1990, 158-59) including:
Other types of fractures that can be described are stellate, a fracture in which lines radiate from the central point of impact; undisplaced, a fracture in which the bones remain in their approximate anatomical position; and greenstick, in which the thick periosteum of sub-adult bones results in bending of one side of the cortex and the fracture of the other (Mann and Murphy 1990, 159).
Conditions such as eburnation and the congenital deformation of bone, e.g. polydactyly (Murphy 2005, 11-12), which do not fall into any of the above categories, can be placed in a separate category termed 'other'.
© Internet Archaeology
URL: http://intarch.ac.uk/journal/issue20/5/04_4.html
Last updated: Wednesday 8th November 2006