
Figure 26: Photograph showing left and right radius belonging to Tom
When examining skeletal remains, evidence of pathology can be uncertain. Some diseases leave no observable trace on the skeletal system. However, given enough time and severity in the living body, most fractures and many of the chronic infectious diseases do leave osteological evidence of their antemortem existence.
Where morphological signs of pathology are apparent, confirmation of the underlying cause is not always absolute. Generally evident, is the response of the skeletal system to the disease. Osteitis, for example, is a general term describing inflammation of bone tissue caused by infection or injury and has no specific cause. Many diseases may elicit similar reactions from bone, and each person may respond to a disease in a different manner.
When examining skeletal remains for indications of pathology, it is most important to give as full a description as possible of any osteological evidence (including photographs). From such observations, extrapolations as to the likely cause of pathology may be possible. Amongst the Pandora skeletal remains, evidence of disease was observed. The pathology of each skeleton from Tom, Dick and Harry is described separately in this section.
The majority of the skeletal remains belonging to Tom were recovered during the 1997 expedition to the Pandora wreck. Consequently, much of this material has remained contained and undisturbed in conservation for the duration of this project, making any examination difficult. However, this material displayed some obvious signs of pathology. Several bones demonstrated abnormal curvature. These included:
The left tibia and fibula demonstrated curvature - both laterally convex. The matching right tibia was highly degraded with both proximal and distal ends removed, leaving only a suggestion that abnormal curvature of the bone was originally present. The right fibula was curved in much the same manner as the left fibula, laterally convex. Both radius and ulna of each forearm curved away in the mid-forearm area, and strongly toward one another to complete an apparently normal distal radio-ulnar joint. A similar curvature is normally expected in a skeleton, but not to the degree seen in the forearm bones of Tom. Neither left nor right humerus demonstrated any abnormal curvature. The left and right femur were also within normal anatomical limits.
Figure 26: Photograph showing left and right radius belonging to Tom
X-ray analysis of the left and right ilium and frontal bones (Figure 62) from this skeleton showed features of some slight interest. The diploe of the reconstructed frontal bone fragments demonstrated small isolated patterns of porosity. This was best described as a 'moth-eaten' appearance. The same feature was also evident in X-rays of both left and right ilium. It could, however, be entirely explained by taphonomic processes, and have no relevance to any disease process present antemortem.
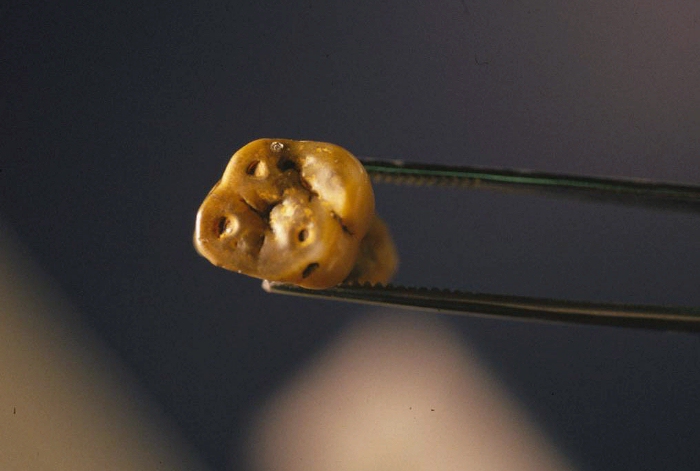
Figure 27: Superior view of a molar tooth. Note the exposure of the pulp cavities.
Teeth from the mandible and right maxillary fragment had been worn down to such an extent that the internal pulp cavities were exposed, which led to pulpitis. Caries was evident on other teeth. Recession of bone on the alveolar processes was also seen, indicating the presence of periodontitis.
Inspection of the sacrum revealed an incompletely fused median process on the dorsal surface of sacral segments 1, 2 and 3.

Figure 28: Dorsal surface of the 3rd and 4th sacral segments - note that it is incompletely fused.
The radius and ulna curvature could be explained from physique alone. Individuals of great musculature have their bones remodelled accordingly, often leaving normal curvatures and muscular markings accentuated. Many parts of Tom's skeleton demonstrated large robust bones, and prominent muscular markings, indicating this individual was very well built.
The tibia and fibula, however, generally do not curve laterally in response to increased musculature. Curvature of these bones is generally the result of a decreased ability of the bone to retain its normal anatomical shape under constant weight stresses from of the upper body, resulting in strain. An anterior bending of the tibia (known as 'saber' tibia) may result from venereal diseases such as syphilis and yaws. A lateral bending of the tibia, observed in this case, is more consistent with rickets, a disease resulting from long-term vitamin D deficiency during skeletal development. Rickets results in the structural weakening of the bones, usually affecting the long bones of the lower limbs first. If rickets causes abnormal bending of the tibia and fibula, it is almost always accompanied by a similar bending in the femur. Cases where rickets has affected the lower limb rarely, if ever, cause bending in the tibia and fibula and not the femur. Generally, in the case of rickets, all of the lower limb long bones are affected because they are weight bearing. This skeleton did not demonstrate any abnormal curvature of either left or right femora.
The 'moth-eaten' appearance evident in X-rays of the frontal bone and ilium could have originated from one of several types of venereal disease, namely syphilis and yaws. On the limited evidence observed in this case, and in the absence of any further molecular studies on the remains, it is difficult to ascertain specifically which of these, if any, were sustained antemortem. Rickets can also affect the skeleton in a similar fashion.
The incompletely fused dorsal region of the sacrum was probably due to the development of a type of spina bifida. During the third and fourth weeks of embryonic life, the neural groove, which runs along the back of the embryo, fuses to form the neural tube. This tube marks the beginning of the development of the spinal cord. Spina bifida occurs when closure of this neural tube is incomplete, and is accompanied by a similar defect in the spinous processes of the affected region of the vertebrae, in this case, the sacrum. The site most often affected is the lumbosacral region, and occasionally it affects higher regions of the vertebral column.
There are three main types of spina bifida, spina bifida occulta, meningocele and meningomyelocele. Spina bifida occulta, the least severe form, results from incomplete fusion of the bony vertebral arch and is usually of less medical significance. The other two varieties of spina bifida can be far more serious and are often incompatible with life. The unfused sacral segments from this skeleton were consistent with the development of spina bifida occulta. It is likely Tom was unaware of this trait and it had no adverse affect on his life at all.

Figure 29: Photograph showing unfused neural arch on the posterior surface of the 1st sacral segment (indicative of spina bifida occulta)
[MA6418-2 also MA6418-3]
The dental infections and associated periodontitis seen on the mandible and right maxillary fragment, although relatively mild, were more than likely the result of poor dental hygiene. The agents of such infection are usually large colonies of various types of bacteria.
In summary, the skeletal remains of this individual indicated the practice of poor dental hygiene. There is a possibility the remains demonstrated evidence of systemic infection, perhaps associated with a venereal disease, or even rickets [see MA6468]. In addition, this individual retained a developmental abnormality known as spina bifida occulta, of which he was probably unaware.
Some of this skeleton was discovered in 1986 and returned to the wreck in 1991. Therefore, a complete examination of the skeletal material was not possible. In the report by Wood and Hodgson (1996), there was no clear evidence of any pathology with the exception of probable periodontal disease. Wood and Hodgson (1996) also made note of a series of terminally located Harris lines seen in an X-ray of the distal left humerus. This indicated some form of environmental stress during the latter stages of adolescence.
Of the skeletal material available for this project, there was some evidence of periodontitis of the lower jaw. Some of the teeth retained a hardened form of dental plaque. In general, the few teeth remaining in the mandible were in exceptional condition, with no evidence of caries.
The spinous processes for the thoracic vertebrae were small, seemingly under-developed and often curved outside the median plane. This curvature was not consistently to the left or right, but rather in an apparently random manner. This feature was of unknown origin and probably of no significance to the individual. There were no other signs of disease on any of the other postcranial bones.
Of the skeletal material belonging to Harry, several indications of possible pathology were evident. The vast majority of pathologically related characteristics were observed on the cranium and mandible, and are discussed below. Very little of the postcranial skeleton was recovered, and abnormal skeletal features were only observed in one instance.
The left radius showed a small localised region of surface porosity, on the medial surface of the mid-shaft. Developmental and pathological features of the cranium and mandible worth noting are summarised as follows:
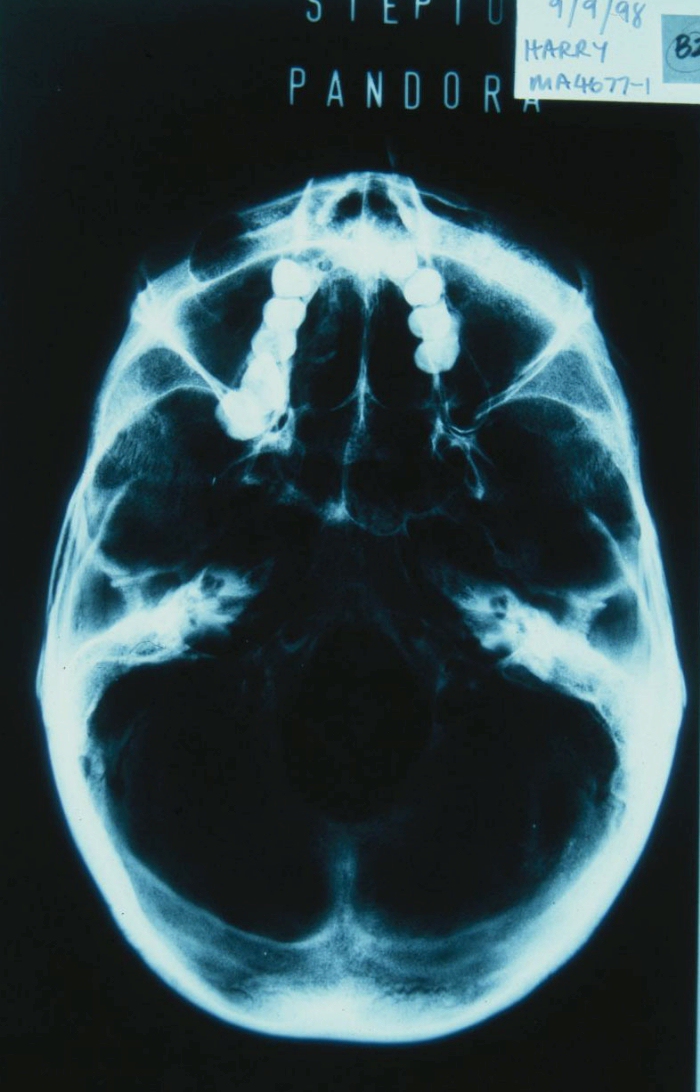
Figure 30: X-Ray of the inferior region of Harry's skull
X-rays of the cranium, mandible and postcranial bones did not appear to show any further evidence of a pathological state.
The origin of the localised porosity seen on the left radius cannot be determined. It is possible this feature related to the same pathological state causing the other abnormalities. The complete cranium belonging to Harry exhibits several interesting characteristics. An abundance of such characteristics are not considered common. Whether they were of pathological origin, or developmental in nature, remains in question.
Considering the mandible first, the degree of atrophy of the left coronoid process and the asymmetry of the mandibular angles is not normal. Abnormalities observed in the temporomandibular joint (TMJ) are probably related to this. The bony infection on the left labial surface of the mandible was caused by an untreated tooth infection passing through the root cavity of the 2nd left molar. This would have caused great discomfort to the individual. It is highly unlikely that this infection alone caused any of the pathological traits in the left ramus of the mandible. In fact, it is possible that the tooth cavity persisted as a secondary infection to the pathology causing the developmental deformities seen on the ramus. The mandible has responded to a long-lasting stress, mostly evident on the left side.
Collectively, the abnormal traits of this skull suggest exposure to a form of long-term stress. As a young adult, the gross features of the skull are fully developed; such extensive narrowing of the maxilla is unlikely to have occurred at this stage in life. Many of these features appear to be developmental, occurring at a young age when the skull was still growing.
The literature describes many pathological states that can affect the skeletal system. Such diseases are usually at the late secondary, or more often tertiary, stage before any cranial expression of the disease is evident. The postcranial skeleton is generally affected before the cranium, which does not appear to be the case with Harry.
Syphilis, a venereal disease, is known to affect the skeletal system, including the cranium, in its late secondary or tertiary stages. If left untreated for an extended period of time, syphilis causes severe disfigurement of the skeletal system and eventual death. If the subject survives the disease long enough, the result can be a cranium with large holes. Clearly, Harry did not live in such a state. The cranium, although apparently pathological, is far from severely disfigured, and the postcranial skeleton is relatively normal.
Late congenital syphilis, is an example of a pathological state which is known to have symptoms which could parallel the cranial abnormalities evident in this skull. A brief list summarising some of the clinical symptoms is given below (Mandel et al. 1990, 1802).
Hutchkinson's incisors can be a good indicator of congenital syphilis. Harry's cranium, however, has lost all upper and lower incisors postmortem. Mulberry molars occur where the 2nd molar tooth has a small rounded crown. They do not appear to be present in Harry's dentition. The cranium did not have obvious frontal bosses. Harry's skull does show exhibit a short maxilla, distorted nasal bones, protruding mandible and a high palatal arch. It is unlikely that Harry's nose was broken traumatically antemortem, as the entire nasal aperture on both sides can clearly be seen to distort in the same manner as the nasal bones from the anterior view.
These signs may provide an explanation for the abnormal cranial characteristics evident in Harry's skull. An infant infected with congenital syphilis does not usually live for a period exceeding 6-8 months (Mandel et al. 1990, 1802). If, however, the child survives this stage, they can live to an age greater than 40. Considering his age, it is therefore possible Harry suffered from late congenital syphilis, although not severely. This could provide one explanation for the developmental traits evident in the cranium and mandible, which began at an early age and persisted into later life.
In summary, it is the authors' opinion that the developmental abnormalities observed on the left ramus of the mandible and TMJ originated from a long lasting pathological state (of soft tissue). Harry's advanced dental caries and the associated bony abscess was likely related (perhaps secondary to) the pathology of the left side of the mandible. Assuming this to be true, major pathology on what could be called the left side of the individual's face might suggest that some, or many, of the other abnormal features of the cranium, were associated with the same pathology. However, this cannot be ascertained with any degree of certainty and it is quite possible the interesting nature of Harry's skull could be accounted for by genetic variation alone.
© Internet Archaeology
URL: http://intarch.ac.uk/journal/issue11/4/29.html
Last updated: Thu Mar 28 2002
{kind=link}
{kind=link}
{kind=link}